Finding out you’re pregnant brings a rush of emotions. Hope, excitement and maybe a little nervousness. So when something goes wrong in those early weeks, it can feel confusing and frightening.
Ectopic pregnancy is one of those early pregnancy complications that many people haven’t heard much about until it happens to them or someone they know.
Understanding what it is, why it happens and what to expect can make a real difference. Knowledge reduces fear. It helps you ask the right questions and recognize warning signs early.
What Is an Ectopic Pregnancy?
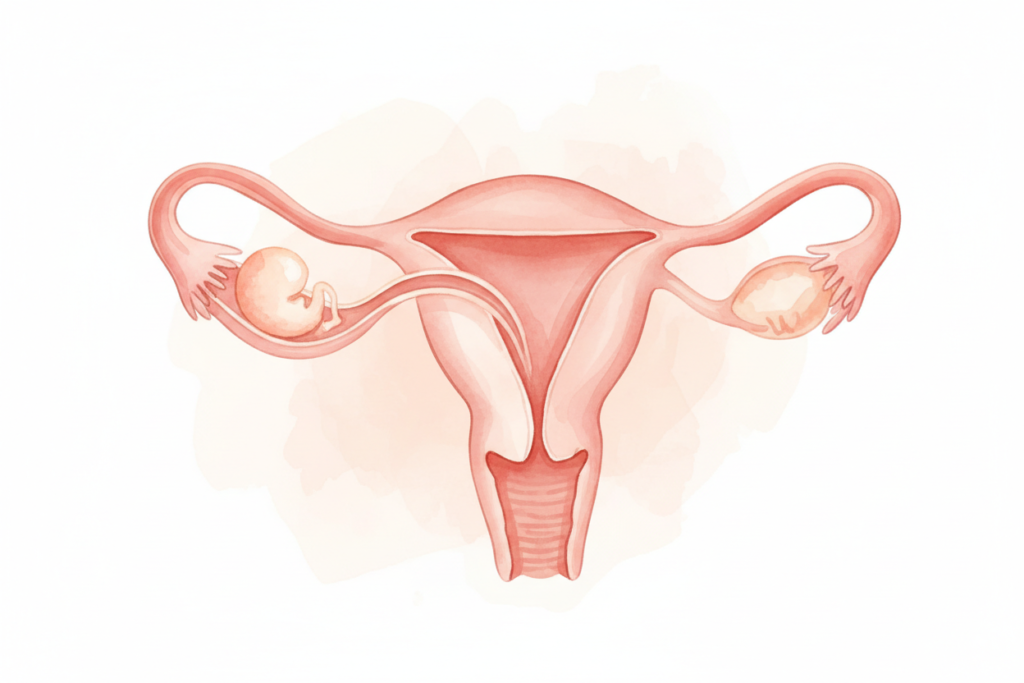
In a normal pregnancy, a fertilized egg travels through the fallopian tube and implants in the uterus. That’s where a baby grows and develops.
In an ectopic pregnancy, the fertilized egg implants somewhere outside the uterus. Most of the time this happens in a fallopian tube. Occasionally it happens in the ovary, cervix or abdominal cavity.
The word ectopic comes from a Greek word meaning out of place. That’s exactly what it is. A pregnancy growing in the wrong location.
The problem is that only the uterus is designed to grow and support a developing pregnancy. A fallopian tube can’t expand the way a uterus can. As the pregnancy grows, it puts dangerous pressure on surrounding tissue.
An ectopic pregnancy cannot survive or develop into a healthy baby. And without treatment it can become a serious medical emergency.
Why Does Ectopic Pregnancy Happen?
This is the question most people want answered. Why does the fertilized egg end up in the wrong place?
The journey from fertilization to implantation takes about three to four days. The egg travels down the fallopian tube using tiny hair-like structures called cilia that gently push it along. Subtle muscle contractions in the tube also help move it forward.
When something disrupts this journey, the egg can get stuck before reaching the uterus.
Damage or scarring inside the fallopian tube is the most common reason. Scarred tissue creates obstacles that slow or stop the egg’s movement. By the time it stops moving, it’s already started to implant wherever it is.
Previous infections are a major cause of this scarring. Pelvic inflammatory disease (PID), often caused by untreated sexually transmitted infections like chlamydia or gonorrhea, can damage the delicate lining of the tubes over time.
Previous surgery on or near the fallopian tubes also increases risk. Scar tissue from surgery can narrow the tube or change its shape.
Sometimes there’s no obvious cause. The egg simply doesn’t make it to the uterus and nobody fully understands why.
Who Is at Higher Risk?
Ectopic pregnancy affects about one to two percent of all pregnancies. Anyone who can get pregnant can have an ectopic pregnancy. But certain factors increase the risk.
Previous ectopic pregnancy is the strongest risk factor. If you’ve had one, your risk of having another is significantly higher.
A history of pelvic inflammatory disease or STIs raises risk because of the scarring effect on fallopian tubes.
Previous pelvic or abdominal surgeries, including appendix removal, can create scar tissue near the tubes.
Endometriosis affects how tissue grows in and around reproductive organs and can change tube function.
Fertility treatments like IVF don’t eliminate ectopic risk. In some cases the risk is slightly higher.
Smoking has been linked to ectopic pregnancy. It may affect how the fallopian tube moves and functions.
Age over 35 slightly increases risk though ectopic pregnancy happens at all ages.
Having risk factors doesn’t mean you will have an ectopic pregnancy. It just means being extra aware of early warning signs.
“Knowing your risk factors isn’t about living in fear. It’s about staying informed and seeking help quickly if something doesn’t feel right.”
Recognizing the Symptoms
Ectopic pregnancy typically shows symptoms between four and twelve weeks of pregnancy. Sometimes earlier.
The tricky part is that early symptoms can feel similar to a normal pregnancy. A missed period, tender breasts and nausea are common in both.
But ectopic pregnancy often brings additional warning signs.
Pain on one side of the abdomen. This is one of the most common early signs. It might feel like a dull ache or a sharp pain. It can come and go at first.
Vaginal bleeding. This is often lighter or different from a normal period. It might look brown or pinkish rather than bright red.
Shoulder tip pain. This is an important one that many people don’t expect. Pain at the tip of your shoulder, especially when lying down, can indicate internal bleeding irritating the diaphragm. This needs immediate attention.
Dizziness or feeling faint. This can happen if internal bleeding is occurring.
Feeling of pressure in the rectum. Some women describe this as needing to use the bathroom urgently without being able to.
If the fallopian tube ruptures, pain becomes severe and sudden. Dizziness, pallor and feeling extremely unwell can follow quickly.
Any of these symptoms in early pregnancy need immediate medical attention. Don’t wait to see if they improve on their own.
A Real-Life Example
Shreya was 29 and had been trying to get pregnant for several months. When she got a positive pregnancy test, she was thrilled.
About a week later, she started feeling a dull ache on her right side. She assumed it was normal stretching and growing pains. She’d read about early pregnancy discomfort and thought this was it.
Two days later the pain was stronger. She noticed some light spotting, which worried her. Her husband suggested she call her doctor.
Shreya wasn’t sure whether to go to the emergency room or wait for a regular appointment. The pain wasn’t unbearable yet. She felt okay in herself.
But something felt off. She decided to go to the hospital.
An ultrasound confirmed an ectopic pregnancy in her right fallopian tube. Because she came in before any rupture, she was treated with medication that stopped the pregnancy from developing further. She didn’t need surgery.
Her doctor later told her that waiting even another day could have changed the outcome significantly. The tube had been close to rupturing.
Shreya recovered well physically. She and her husband were counseled about future pregnancy and the slightly higher risk of another ectopic. Fourteen months later she had a healthy pregnancy that developed normally in her uterus.
Her story is one many women share. Coming in early made all the difference.
“Early detection isn’t just important in ectopic pregnancy. It’s everything. The sooner it’s found the more treatment options are available and the safer the outcome.”
How Ectopic Pregnancy Is Diagnosed
If your doctor suspects an ectopic pregnancy, they’ll usually start with a blood test and an ultrasound.
The blood test measures hCG, the pregnancy hormone. In a normal pregnancy, hCG levels roughly double every 48 to 72 hours. In an ectopic pregnancy, levels often rise more slowly or plateau. Repeated tests over a couple of days give valuable information.
A transvaginal ultrasound is usually more accurate than an abdominal one in early pregnancy. It allows doctors to see whether there’s a gestational sac inside the uterus.
Not seeing a sac in the uterus when hCG levels are high enough to show one is a strong indicator of ectopic pregnancy.
Sometimes the ectopic is visible on the scan directly. Other times it’s suspected based on a combination of symptoms, blood work and what’s absent rather than what’s present.
Diagnosis can take more than one visit and more than one test. This can feel frustrating when you’re anxious for answers but it’s important to have enough information to act safely. Treatment Options
Treatment depends on several factors. How early it’s caught, whether the tube has ruptured and the woman’s overall health and future pregnancy plans.
Medication. Methotrexate is a drug that stops the pregnancy tissue from growing. It’s given by injection. The pregnancy tissue then gradually breaks down and is absorbed by the body. This option works best when the ectopic is caught early and hasn’t ruptured. It avoids surgery but requires follow-up blood tests to ensure it’s working.
Laparoscopic surgery. If medication isn’t suitable or the tube has ruptured, surgery is needed. A laparoscopy is a minimally invasive procedure using small incisions and a camera. The surgeon removes the ectopic pregnancy. Depending on the tube’s condition, they may save it or remove it entirely.
Emergency surgery. If there’s been a rupture and internal bleeding is significant, emergency surgery is needed. This is more serious but life-saving.
Your treatment team will guide you through the options that make sense for your situation. There’s no one-size-fits-all answer
The Emotional Side Nobody Talks About Enough
An ectopic pregnancy is a pregnancy loss. Even though it couldn’t have continued safely, it was still a wanted pregnancy for most people. The grief that follows is real.
Many women describe a strange kind of loss. They feel they need to be grateful they’re physically okay while also grieving the pregnancy that wasn’t. Both feelings are valid. They can exist at the same time.
Partners grieve too. But sometimes don’t know how to express it or feel their grief is less important. It isn’t.
Some women feel fear about future pregnancies. Anxiety about whether it will happen again. Worry about whether they can still get pregnant at all.
These feelings are normal. They don’t mean something is wrong with you. They mean you were invested in a pregnancy you hoped for.
Counseling or talking to others who’ve been through it can help. Many hospitals have support services. Online communities for pregnancy loss are also available where people share experiences with compassion and understanding.
“Grieving an ectopic pregnancy is not only normal. It’s healthy. Allow yourself to feel what you feel. Healing takes time and that’s okay.”
Future Pregnancy After Ectopic
One of the first questions people ask after treatment is whether they can get pregnant again.
For most women the answer is yes. Especially if one fallopian tube is healthy and functioning.
If one tube was removed, the remaining tube can still carry eggs to the uterus. Many women go on to have healthy pregnancies with one tube.
If both tubes have been affected, IVF is an option. During IVF, fertilization happens outside the body and the embryo is placed directly into the uterus, bypassing the tubes altogether.
Your doctor will advise waiting a period of time before trying again, usually around three months after methotrexate treatment. This gives your body time to recover and ensures the medication has fully cleared your system.
Future pregnancies will be monitored more carefully with early ultrasounds to confirm the location of implantation. This is precautionary and reassuring.
Many women who’ve had an ectopic pregnancy go on to have healthy full-term pregnancies. Shreya’s story above is one of many.
When to Seek Immediate Help
It’s worth being very clear about when to go to the emergency room without waiting.
Go immediately if you experience:
Sudden severe abdominal pain that doesn’t ease. Pain at the tip of your shoulder. Feeling faint, dizzy or collapsing. Heavy vaginal bleeding. Feeling very unwell with any combination of the above.
These can be signs of a ruptured ectopic pregnancy. This is a medical emergency. Time matters significantly.
If you’re in early pregnancy and feel unsure about any symptoms, it’s always better to be assessed and reassured than to wait at home. Doctors and nurses would rather see you unnecessarily than have you delay when it’s serious.
Trust your instincts. If something feels wrong in early pregnancy, get it checked.
Reducing Your Risk
You can’t always prevent an ectopic pregnancy. But you can reduce some of the risk factors.
Getting tested regularly for STIs, especially if you’re sexually active with new or multiple partners, helps catch infections before they cause tubal damage. Chlamydia in particular often has no symptoms but can silently damage fallopian tubes over time.
Using protection consistently reduces STI risk. Treating infections promptly prevents them from progressing to pelvic inflammatory disease.
If you smoke, stopping is beneficial for many aspects of reproductive health including ectopic pregnancy risk.
If you’ve had a previous ectopic pregnancy, discuss early monitoring with your doctor when you’re trying to conceive again.
These steps can’t eliminate risk entirely. But they address the most common controllable causes.”You can’t control everything about your reproductive health. But you can stay informed, act early and trust your body when something doesn’t feel right.”
Final Thoughts
Ectopic pregnancy is a serious complication but it’s also one where early detection genuinely changes outcomes. Most women who receive prompt treatment recover well and go on to have healthy future pregnancies.
The most important thing is awareness. Knowing what symptoms to watch for in early pregnancy. Knowing that shoulder pain and one-sided abdominal pain deserve attention. Knowing that it’s always better to get checked than to wait.
If you’ve been through an ectopic pregnancy, be patient with yourself. Physical recovery takes weeks. Emotional recovery often takes longer. Both timelines are valid.
If you’re trying to conceive again after an ectopic, work closely with your healthcare provider. Early scans and monitoring give reassurance and catch any problems quickly.
Your body is resilient. With the right care and information you can navigate this with as much confidence and calm as possible.
You don’t need to have all the answers. You just need to know when to seek help and trust that asking questions is always the right thing to do.